


Feature
Is Our Air Deadly?
Increased air pollution is correlated with hazardous health effects. What is happening and why?
Dr Janine Clemons
Many factors, either natural or man-made, contribute pollutants to the air. As industrial growth occurs alongside a raised standard of living and increased consumption of combustible fossil fuels, most of the observed decrease in air quality can be attributed to man-made sources -- cars and other vehicles, wood burners and industry.
Increasing concerns regarding New Zealand's air quality is founded in recent medical reports stating that elevated level of certain pollutants in urban communities correlates well with the incidence of air-pollution-related human health effects in susceptible populations such as the elderly. These pollutants include particulate matter (PM), carbon monoxide (CO), sulphur dioxide (SO2) and nitrogen dioxide (NO2). New Zealand's use of automotive diesel engines and wood burners are acute sources of PM, SO2, CO, and NO2 in the air.
An important contributor to urban air pollution is the continually rising vehicle ownership. The main cause of the decrease in Auckland's air quality is the city's increased emission of incompletely combusted fossil fuel from car exhaust. Globally, preventative measures such as charcoal canisters, catalytic converters, unleaded gasoline, and ethanol additives to gasoline, have helped decrease vehicle emissions. However, these preventative measures are not as effective in New Zealand because:
- it is necessary to legislate the installation of these devices to prevent emissions
- these preventative measures are less effective in normal, idling, urban traffic typically found at high levels in the North Island
In the South Island, a more substantive player in increased PM loading is the use of domestic wood burners in the winter as the major source of heat. Winter air quality in Christchurch is an issue due to a culmination of factors: temperature inversions, winter wind patterns and geographical location. These combine to cause PM levels to be considerably higher than the acceptable standard.
Standard air quality testing includes monitoring CO, SO2, O3, lead, total hydrocarbons and sometimes benzene. However, the increased particle concentration in the air and the potentially carcinogenic and toxic agents bound to PM, are only recently being considered here, in contrast to the significant focus on PM worldwide. Within the last year, the U.S. Environmental Protection Agency has focused particularly on the hazard of PM less than 10 mm (PM10) and 2.5 mm (PM2.5) to children, a group of the population where asthma mortality is on the increase. To no lesser degree, the elderly and persons with pre-existing medical conditions are also at increased risk.
Standardised air quality monitoring is complex due to the number of variables associated within a country, city, community or individual. However, generalised monitoring is possible for contaminants known to be present at significant levels worldwide and known to have adverse health effects. High levels of SO2, O3, NO2, PM10, and CO are all known to be toxic at a certain concentration.
In New Zealand, guidelines are adapted and modified from those published by the World Health Organization in 1987 to control ambient levels of these pollutants. The guidelines are based on an established combination of sentinel health effects for the individual air pollutants, but, because particulate material is so complex, WHO has been reluctant to state guidelines of acceptable PM levels.
Particulate Toxicity
The task of assigning risk to the New Zealand population is very difficult because of the widely diverse mechanisms of toxicity for all the components in air pollution. However, this article will focus on PM toxicity as PM is a contaminant of concern to New Zealanders because of its significantly increased levels compared to guidelines.
The issue of PM's adverse health effects is controversial, with diverse scientific perceptions of the problem. Some scientists focus on the actual level of PM, since at high concentrations it appears to relate to an increase in specific respiratory diseases. Yet other researchers are more concerned with the chemical components adhered to the particulates, including the organic (e.g. polycyclic aromatic hydrocarbons (PAH)) inorganic (e.g. metals), and gaseous (e.g. SO2) elements. Recently it is becoming clear that the negative health effects are likely due to the mixture of all these variables, together producing complex synergistic or antagonistic interactions.
Air PM consists of a multiplicity of potentially harmful constituents. Within PM there are two very different, yet equally dangerous, variables:
- active particulate characteristics
- chemical identification and levels of the adhered organic and inorganic compounds
Hence, there is a divergence in the type of toxicity studied when examining the adverse health effects associated with PM. One field of research examines the levels and toxicity associated with the organic components (PAH) adhering to PM that are known, in part, to be highly carcinogenic. Their carcinogenicity is due to their high degree of affinity to DNA, which can either cause mutations in the sequence, gaps, or strand breaks and/or irreversible binding to the DNA thereby altering normal gene expression (hence the term genotoxic compounds).
The organic component of PM has not only been shown to be genotoxic, but also to have endocrine-disruptive properties. Environmental endocrine-disrupting compounds (EDC) are broadly defined as "exogenous substances that cause adverse health effects in an intact organism, or its progeny, secondary to changes in endocrine function".
One premise behind endocrine disruption is that substances may mimic endogenous hormones by eliciting similar effects or by blocking or diminishing their function by competing for available receptor sites. Multi-ring organics such as PAH, have been implicated as EDCs.
One proposed mechanism-of-action is via a protein receptor, the aromatic hydrocarbon receptor (AhR), which combines with the chemical contaminant signalling DNA pathways to produce anti-estrogenic effects, actions that oppose normal estrogen responses.
Previous studies examining the effects of industrial gas plant residue, known to contain high levels of PAH, implicate this type of air particulate material in causing significant anti-estrogenic activities. Only recently have we identified certain PAH as "estrogenic" where the compounds mimic normal estrogenic responses instead of antagonise them.
Both organic and inorganic components of PM culminate in the respiratory system, the target organ for PM10 toxicity. Larger particulate material (2.5 mm) reaches the larger bronchi while the smaller particles (.5 mm) are able to enter the alveolar sacs of the lungs. Exposure to particulate potentially influences functions of the respiratory tract, including gas exchange, metabolism, immunity and sense of smell.
The size, shape, surface chemistry and dissolvable components are the major determinants of particle toxicity. The responses of the lung may include inflammation, asthma, ulceration, oedema, fibrosis and cancer. In other words, the complexity of particulate-induced lung toxicity is due to the combination of particulate structure and composition. Recent research examines the mechanism behind the particulate-induced inflammation leading to chronic respiratory injury such as allergic asthma.
The Canterbury Regional Council (CRC) has identified Christchurch as having one of the worst air quality problems in New Zealand, rivalling that of London or Birmingham. Although Auckland's larger population and greater car traffic produces a high level of diesel- and petrol-related PM, its topography and constant sea breeze mitigates the build-up of dangerously high levels of PM, CO, SO2, NO2, or O3. Consequently, the CRC has made a considerable effort to inform the public of the source and occurrence of the high incidence of PM in response to public concerns about air pollution.
One strategy has been to propose banning the use of domestic coal ban in specified areas in the city. However, the CRC does recognise that the toxicity of Christchurch's air pollution is still ongoing. Although it is hypothesised that PM in combination with other contributing factors may explain the high incidence of respiratory-related complaints, no real toxicological characterisation has yet been performed.
Chemical monitoring of the PAH levels within PM is a current CRC initiative, but this needs to be combined with biological and health effects monitoring to fully define the risks associated with Christchurch's woodsmoke, diesel and industrial exhaust, and refuse and paddock burns.
New Zealand's "clean, green image" reputation helps support the country's economy. Certainly the issue of decreased air quality is discordant with this image and needs to be rectified, not unlike how the CRC is currently tackling Christchurch's unacceptable wintertime air pollution.
Toxicological and chemical characterisation of the pollution is necessary to orient scientists and officials to the cause and/or mitigation of observed adverse health effects in the New Zealand population.
Compared to other industrialised nations, our pollution problems may seem of a manageable scale, but it is important that they are contained or prevented.
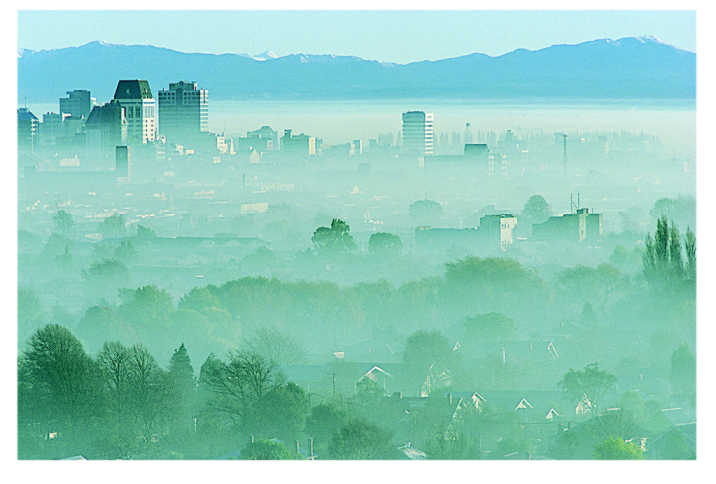
Buildings loom out of the morning smog in Christchurch. Photo used by permission of the Canterbury Regional Council.
Dr Janine Clemons is an Environmental Toxicologist working on the Ecotoxicology Program at Landcare Research
All contents of this site copyright © 1990-2007 Webcentre Ltd. All Rights Reserved